Healthcare revenue cycle data sits at the intersection of clinical operations and financial performance. Every patient encounter generates a cascade of administrative transactions — charge capture, claim submission, adjudication, remittance, denial management, and patient billing — each producing structured data that healthcare organizations must capture, store, and analyze to sustain financial health.
For health systems, revenue cycle data is the primary indicator of operational efficiency and financial viability. For payers, it drives payment integrity and fraud detection. For data architects and engineers building healthcare analytics platforms, revenue cycle data presents unique modeling challenges: high transaction volumes, complex business rules, multi-version claim histories, and the need to support both operational reporting and strategic analytics simultaneously.
This guide covers everything a healthcare data architect, data modeler, or data engineer needs to know about revenue cycle data — from core data elements and EDI standards to production-ready data model design for Snowflake, Databricks, and BigQuery.
What Is Healthcare Revenue Cycle Data?
The revenue cycle is the complete set of administrative and clinical functions that contribute to the capture, management, and collection of patient service revenue. Revenue cycle data is the structured record of every transaction in this process — from patient registration through final payment collection.
Revenue cycle data spans several operational domains:
Patient access data captures the front-end revenue cycle including patient registration demographics, insurance verification results, prior authorization approvals, and financial counseling interactions. Front-end data quality directly determines downstream claim accuracy — registration errors cause eligibility denials that cannot be resolved without correcting the source data.
Charge capture data records every billable service, supply, and procedure delivered during a patient encounter before claim submission. The charge master is the reference database linking clinical documentation to billable revenue codes, CPT codes, and standard charges. Incomplete charge capture results in permanent revenue loss that cannot be recovered after timely filing deadlines expire.
Claims transaction data encompasses the complete lifecycle of claim submission through adjudication — the EDI 837 claim transaction, clearinghouse validation results, payer adjudication outcomes, and EDI 835 remittance advice payments. Claims transaction data is the core of revenue cycle analytics.
Denial management data tracks claims that were not paid as expected — capturing denial reason codes, appeal submissions, appeal outcomes, and final resolution. Claim denial analytics identify systemic billing problems that require upstream process improvement.
Accounts receivable data captures the aging and collection status of outstanding balances from payers and patients — the financial heartbeat of the revenue cycle that determines cash flow and collection effectiveness.
Patient financial data includes patient statements, payment plan arrangements, financial assistance applications, and collection activity — representing the patient-facing dimension of the revenue cycle that increasingly drives total collections as patient cost-sharing grows.
Core Revenue Cycle Data Elements
Every healthcare data team working with revenue cycle data needs to understand these fundamental fields:
The claim adjudication (clm_adj) status captures the payer determination on each claim — paid, denied, pending, or adjusted — and drives the entire denial management and accounts receivable workflow.
The claim denial reason (clm_denial_rsn_cd) uses standardized CARC codes from the EDI 835 remittance to explain why a claim was not paid. Denial reason code analytics identify the highest-volume denial categories driving revenue leakage.
The days in accounts receivable (days_ar) measures revenue cycle collection velocity — the average number of days from service delivery to cash collection. Industry best practice targets under 40 days for physician practices and under 50 days for hospitals.
The clean claim rate (cln_clm) measures what percentage of submitted claims are accepted on first submission without correction. Leading organizations achieve clean claim rates above 95 percent.
The net collection rate (net_coll_rt) measures the percentage of net collectible revenue actually collected — the most important single metric of revenue cycle performance. Best practice is above 96 percent.
The prior authorization (prior_auth) approval number must be included on claims for services requiring advance approval — missing authorizations are among the most preventable and costly denial categories.
The remittance advice (remit_adv) is the EDI 835 transaction communicating how each claim was adjudicated — the primary data source for payment posting, contractual adjustment calculation, and denial management.
The charge master (chrg_mstr) is the comprehensive price list linking every billable item to revenue codes, procedure codes, and standard charges — the foundation of accurate claim generation.
The contractual adjustment (cntrct_adj_amt) is the difference between billed charges and the contracted allowed amount — the largest single revenue adjustment category in most healthcare organizations.
The denial rate (denial_rt_pct) is the percentage of submitted claims denied during initial adjudication — the primary leading indicator of revenue cycle quality that benchmarks against industry averages of five to ten percent.
Revenue Cycle EDI Standards
Revenue cycle data flows through HIPAA-mandated electronic data interchange standards. Every healthcare data engineer building revenue cycle analytics must understand these transaction sets:
EDI 837 is the electronic claim transaction — 837P for professional claims, 837I for institutional claims, and 837D for dental claims. The 837 carries all claim data elements from patient demographics through procedure codes and billed amounts.
EDI 835 is the electronic remittance advice that communicates adjudication results. The 835 contains Claim Adjustment Reason Codes explaining payment decisions and Remittance Advice Remark Codes providing additional context. Healthcare data teams process 835 transactions to automate payment posting, calculate contractual adjustments, and generate denial work queues. Electronic funds transfer paired with the 835 eliminates paper check processing.
EDI 270/271 are the eligibility inquiry and response transactions used for real-time eligibility verification before service delivery. 270/271 processing is the primary defense against eligibility-related claim denials.
EDI 276/277 are the claim status inquiry and response transactions that allow providers to check adjudication status for submitted claims without calling the payer.
EDI 278 is the prior authorization request and response transaction — increasingly required as CMS mandates electronic prior authorization through FHIR-based APIs for Medicare Advantage plans.
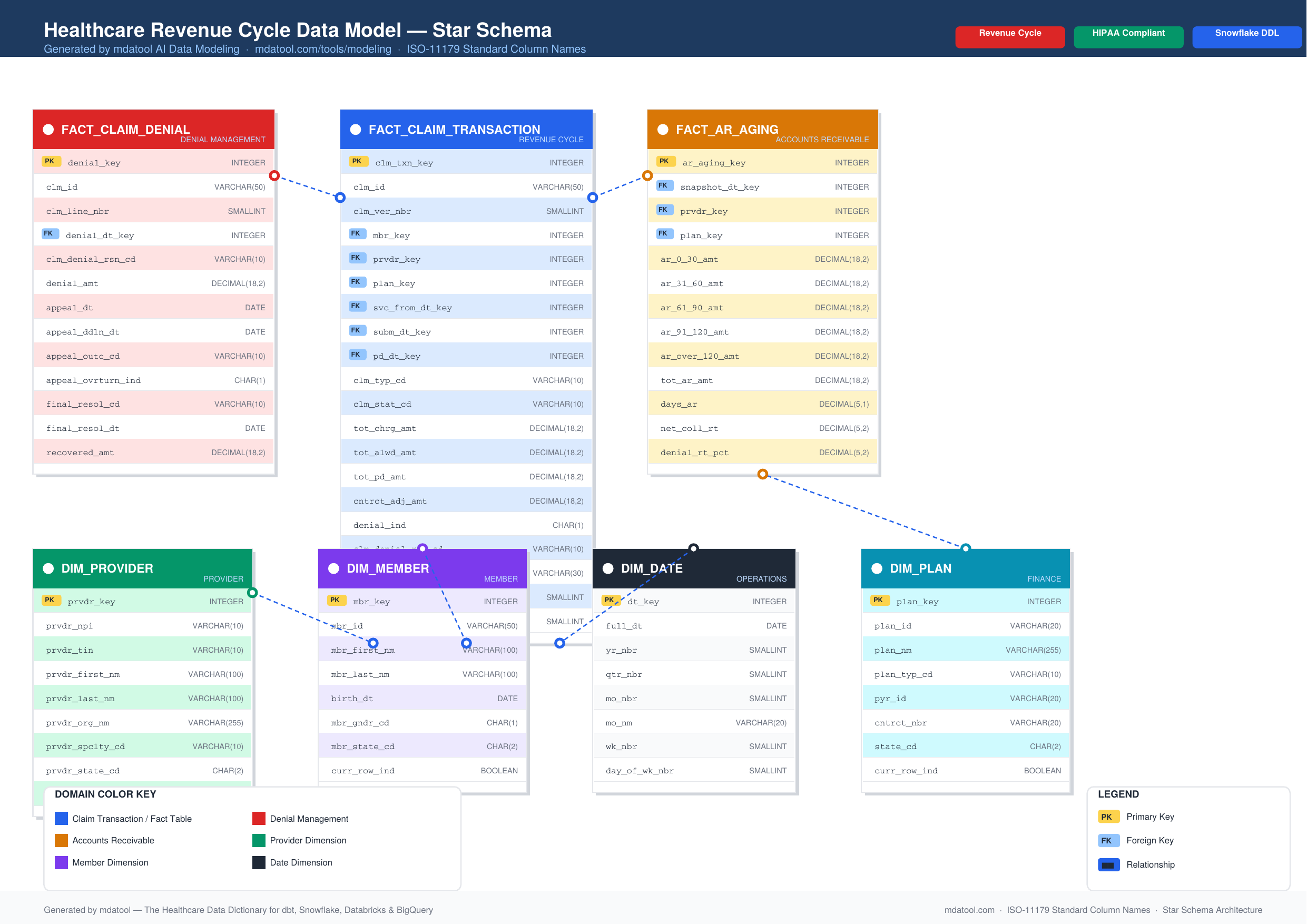
Revenue Cycle Data Model Design
Revenue cycle data warehouses must support multiple analytical grain levels simultaneously — claim header summaries for financial reporting, claim line detail for procedure analytics, and claim version history for denial management. Here is a production-ready revenue cycle data model:
Fact Table: FACT_CLAIM_TRANSACTION
-- Snowflake DDL — generated with mdatool AI Data Modeling
-- mdatool.com/tools/modeling
CREATE TABLE FACT_CLAIM_TRANSACTION (
CLM_TXN_KEY INTEGER NOT NULL, -- surrogate key
CLM_ID VARCHAR(50) NOT NULL, -- claim identifier
CLM_VER_NBR SMALLINT NOT NULL, -- claim version number
MBR_KEY INTEGER NOT NULL, -- FK to DIM_MEMBER
PRVDR_KEY INTEGER NOT NULL, -- FK to DIM_PROVIDER
PLAN_KEY INTEGER NOT NULL, -- FK to DIM_PLAN
SVC_FROM_DT_KEY INTEGER NOT NULL, -- FK to DIM_DATE
SUBM_DT_KEY INTEGER NOT NULL, -- FK to DIM_DATE (submission)
PD_DT_KEY INTEGER NOT NULL, -- FK to DIM_DATE (payment)
CLM_TYP_CD VARCHAR(10), -- claim type (P/I/D)
CLM_STAT_CD VARCHAR(10), -- adjudication status
CLM_FREQ_CD CHAR(1), -- claim frequency code
BILL_TYP_CD VARCHAR(3), -- bill type code
TOT_CHRG_AMT DECIMAL(18,2), -- total billed charges
TOT_ALWD_AMT DECIMAL(18,2), -- total allowed amount
TOT_PD_AMT DECIMAL(18,2), -- total paid amount
CNTRCT_ADJ_AMT DECIMAL(18,2), -- contractual adjustment
TOT_MBR_LIAB_AMT DECIMAL(18,2), -- member liability
TOT_DED_AMT DECIMAL(18,2), -- deductible applied
TOT_COPAY_AMT DECIMAL(18,2), -- copay amount
TOT_COINS_AMT DECIMAL(18,2), -- coinsurance amount
DENIAL_IND CHAR(1), -- denial indicator
CLM_DENIAL_RSN_CD VARCHAR(10), -- primary denial reason
PRIOR_AUTH_NBR VARCHAR(30), -- prior authorization number
CLM_LAG_DAYS SMALLINT, -- days from service to submission
DAYS_AR SMALLINT, -- days from service to payment
LOAD_DT TIMESTAMP_NTZ NOT NULL DEFAULT CURRENT_TIMESTAMP,
CONSTRAINT PK_FACT_CLAIM_TRANSACTION
PRIMARY KEY (CLM_TXN_KEY)
);
Denial Analytics Table
-- One row per denial event per claim
CREATE TABLE FACT_CLAIM_DENIAL (
DENIAL_KEY INTEGER NOT NULL,
CLM_ID VARCHAR(50) NOT NULL, -- claim identifier
CLM_LINE_NBR SMALLINT, -- service line number
DENIAL_DT_KEY INTEGER NOT NULL, -- FK to DIM_DATE
CLM_DENIAL_RSN_CD VARCHAR(10), -- CARC denial reason code
DENIAL_AMT DECIMAL(18,2), -- denied amount
APPEAL_DT DATE, -- appeal submission date
APPEAL_DDLN_DT DATE, -- appeal deadline date
APPEAL_OUTC_CD VARCHAR(10), -- appeal outcome code
APPEAL_OVRTURN_IND CHAR(1), -- appeal overturned indicator
FINAL_RESOL_CD VARCHAR(10), -- final resolution code
FINAL_RESOL_DT DATE, -- final resolution date
RECOVERED_AMT DECIMAL(18,2), -- amount recovered on appeal
LOAD_DT TIMESTAMP_NTZ NOT NULL DEFAULT CURRENT_TIMESTAMP,
CONSTRAINT PK_FACT_CLAIM_DENIAL PRIMARY KEY (DENIAL_KEY)
);
Accounts Receivable Table
-- Daily AR aging snapshot
CREATE TABLE FACT_AR_AGING (
AR_AGING_KEY INTEGER NOT NULL,
SNAPSHOT_DT_KEY INTEGER NOT NULL, -- FK to DIM_DATE
PRVDR_KEY INTEGER NOT NULL, -- FK to DIM_PROVIDER
PLAN_KEY INTEGER NOT NULL, -- FK to DIM_PLAN
AR_0_30_AMT DECIMAL(18,2), -- 0-30 days AR balance
AR_31_60_AMT DECIMAL(18,2), -- 31-60 days AR balance
AR_61_90_AMT DECIMAL(18,2), -- 61-90 days AR balance
AR_91_120_AMT DECIMAL(18,2), -- 91-120 days AR balance
AR_OVER_120_AMT DECIMAL(18,2), -- over 120 days AR balance
TOT_AR_AMT DECIMAL(18,2), -- total AR balance
DAYS_AR DECIMAL(5,1), -- days in AR metric
NET_COLL_RT DECIMAL(5,2), -- net collection rate
DENIAL_RT_PCT DECIMAL(5,2), -- denial rate percentage
LOAD_DT TIMESTAMP_NTZ NOT NULL DEFAULT CURRENT_TIMESTAMP,
CONSTRAINT PK_FACT_AR_AGING PRIMARY KEY (AR_AGING_KEY)
);
Generate this complete schema instantly using the mdatool AI Data Modeling tool — select Finance and Revenue Cycle as your domain, Star Schema as your architecture, and your target platform.
Key Revenue Cycle Analytics
Healthcare data teams build the following core analytics on top of the revenue cycle data model:
Denial Rate Analytics calculate denial rates by payer, denial reason, service line, provider, and facility to identify the highest-volume denial categories and measure improvement from process interventions. The goal is reducing denial rates below five percent of submitted claim volume.
Days in AR Trending tracks accounts receivable aging over time to measure collection velocity. An increasing days in AR trend signals revenue cycle deterioration requiring investigation — common causes include payer processing delays, increased denial rates, or reduced follow-up staffing.
Clean Claim Rate Monitoring measures first-pass claim acceptance rates by payer and billing office. Clean claim rates below 90 percent indicate systematic billing errors requiring registration, coding, or charge capture process improvement.
Net Collection Rate Benchmarking compares actual collections against net collectible revenue by payer and service line to identify payers or service categories where collections are underperforming contractual entitlement.
Prior Authorization Compliance tracks authorization denial rates by service type and payer to identify services frequently billed without required authorization, enabling proactive authorization workflow improvements that prevent avoidable denials.
Denial Root Cause Analysis (rca_denial) maps denial reason codes back to their upstream process origin — eligibility denials to registration workflows, authorization denials to scheduling and utilization management, coding denials to documentation and coding education gaps.
Claim Lag Days Monitoring tracks the time from service delivery to claim submission by department and provider to identify charge capture delays that increase timely filing risk and slow cash flow.
Cost to Collect Analysis measures total revenue cycle operating expense per dollar collected to evaluate operational efficiency and calculate return on investment from revenue cycle technology and staffing changes.
Revenue Cycle Performance Benchmarks
Healthcare data teams use these industry benchmarks to evaluate revenue cycle performance:
| Metric | Best Practice | Average |
|---|---|---|
| Days in AR | < 40 days | 50-55 days |
| Clean claim rate | > 95% | 85-90% |
| Net collection rate | > 96% | 90-93% |
| Denial rate | < 5% | 8-12% |
| First pass resolution | > 90% | 75-85% |
| Cost to collect | < 3 cents/$ | 5-7 cents/$ |
| Point of service collection | > 60% | 30-40% |
| Appeal overturn rate | > 50% | 35-45% |
Revenue Cycle Data Quality Considerations
Revenue cycle data quality issues directly affect financial reporting accuracy and collection effectiveness:
Claim version management is the most complex revenue cycle data quality challenge. Every time a claim is adjusted, corrected, or voided a new claim version is created. Analytics pipelines must identify the appropriate version for each use case — the original version for denial analytics, the final paid version for financial reporting, and all versions for audit trails.
Payment posting accuracy errors create incorrect account balances that misdirect collection efforts. Electronic remittance processing through the 835 transaction eliminates manual posting errors and accelerates cash application, but requires accurate mapping of CARC and RARC codes to denial categories.
Contractual adjustment calculation errors arise when fee schedule tables are not current, causing incorrect allowed amount calculations that overstate or understate expected reimbursement. Regular fee schedule maintenance is essential for accurate net revenue modeling.
Duplicate claim detection prevents double payment for the same service. Deduplication logic must identify duplicate claims across different claim IDs, dates of submission, and adjudication cycles while preserving legitimate multi-line and split-billing scenarios.
Timely filing compliance requires monitoring claim submission dates against payer-specific filing deadlines. The timely filing limit varies by payer from 90 days to 24 months, and missing deadlines results in permanent unrecoverable revenue loss.
Revenue Cycle Data Tools
mdatool provides several free tools for healthcare revenue cycle data work:
- AI Data Modeling — Generate a complete revenue cycle data model for Snowflake, BigQuery, or Databricks in 30 seconds
- SQL Linter — Validate revenue cycle analytics SQL against healthcare naming standards
- DDL Converter — Convert revenue cycle schema DDL between database platforms instantly
- Data Model Canvas — Visualize your revenue cycle schema as an interactive ER diagram with PDF export
- [ICD-10 Code Search](/tools/icd10-search) — Search diagnosis codes used in medical necessity determination
- [HCC Calculator](/tools/hcc-calculator) — Calculate risk scores from diagnosis codes for value-based payment analytics
Frequently Asked Questions
What is the difference between gross revenue and net revenue in healthcare? Gross revenue is the total amount billed to payers and patients at standard chargemaster rates before any adjustments. Net revenue is what the organization actually expects to collect after subtracting contractual adjustments representing the difference between billed charges and contracted allowed amounts, charity care write-offs for financially qualified patients, and bad debt allowances for uncollectible balances. In most healthcare markets, net revenue is 25 to 40 percent of gross revenue due to large contractual adjustments from payer contracts.
What is a clean claim and why does it matter? A clean claim contains all required data elements, passes all payer editing rules, and is accepted for adjudication on first submission without correction. Clean claim rates directly measure revenue cycle front-end quality — billing accuracy, eligibility verification completeness, and authorization management effectiveness. Each percentage point improvement in clean claim rate reduces rework costs and accelerates cash collection. Industry leaders achieve clean claim rates above 95 percent while average performers see 85 to 90 percent.
How are CARC and RARC codes used in denial analytics? Claim Adjustment Reason Codes are standardized codes in the EDI 835 remittance advice that explain why a payment was adjusted or denied. Remittance Advice Remark Codes provide additional context for the adjustment. Healthcare data teams map CARC codes to denial categories — eligibility, authorization, coding, timely filing, and medical necessity — to calculate category-specific denial rates and prioritize process improvement initiatives targeting the highest-volume and highest-dollar denial categories.
What is the difference between a denial and a rejection? A rejection occurs before adjudication when a claim fails technical validation at the clearinghouse or payer intake level due to missing required fields, invalid data formats, or enrollment issues. Rejected claims must be corrected and resubmitted as new claims. A denial occurs after adjudication when the payer processes the claim but determines it does not meet coverage criteria, resulting in non-payment with a denial reason code. Denials can be appealed while rejections require correction and resubmission.
How do you calculate days in accounts receivable? Days in AR is calculated by dividing net accounts receivable by average daily net patient service revenue. For example, if net AR is 5 million dollars and average daily net revenue is 100,000 dollars, days in AR equals 50 days. This metric measures how many days of revenue are outstanding in accounts receivable at any given time. A lower number indicates faster collection. Healthcare data teams calculate days in AR at the organization, payer, facility, and service line levels to identify collection performance variation.
What is the timely filing limit and what happens if it is missed? The timely filing limit is the contractually or regulatorily mandated deadline for submitting a claim to a payer after the date of service. Medicare requires claims within 12 months, commercial payers specify limits in provider contracts ranging from 90 days to 365 days, and Medicaid limits vary by state. Claims submitted after the timely filing deadline are denied as untimely and cannot be appealed unless the provider can demonstrate the delay was caused by circumstances beyond their control. Timely filing denials represent permanent unrecoverable revenue loss — making timely submission monitoring a critical revenue cycle control.
What is prior authorization and what happens when it is missing? Prior authorization is advance approval from a health insurance payer required before delivering specific non-emergency services including elective surgeries, advanced imaging, specialty medications, and certain outpatient procedures. When a required prior authorization is missing at the time of claim submission, the payer denies the claim with an authorization-related denial reason code. While some authorization denials can be retroactively appealed with documentation of medical necessity, many payers deny retroactive authorization requests making missing authorization one of the most costly and preventable denial categories.
mdatool Team
The mdatool team builds free engineering tools for healthcare data architects, analysts, and engineers working across payer, provider, and life sciences data.
Related Guides
Key Terms in This Article
Free Tools
Ready to improve your data architecture?
Free tools for DDL conversion, SQL analysis, naming standards, and more.
Get weekly healthcare data engineering tips
Practical guides on data modeling, SQL standards, and healthcare domain conventions — straight to your inbox.
No spam. Unsubscribe any time.